Canada Knocks Out Flu, U.S. Public Kept In The Dark
June 09, 2010
 By David M. Burd, June 2, 2010
By David M. Burd, June 2, 2010
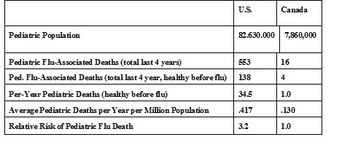
Canada the last four years totaled sixteen "flu-associated" fatalities for their paediatric age category, defined as everybody under 18, and this included all H1N1 and seasonal cases. Three-quarters of these deaths had severe and chronic underlying health conditions, as did the mortality of a similar percentage of adults over 18.
Thus over the last four years Canada averaged but a single paediatric flu-associated death per year (not having severe chronic health issues) among its paediatric population of 7.86 million, Canada's total population being 33 million (Flu statistics are from The Public Health Agency of Canada's Fluwatch website). Importantly, this has taken place with 60% (or more) of their paediatric group remaining unvaccinated.
By comparison, during the same four-year time span starting the flu season of 2006 - 2007, the identical U.S. pediatric group had 553 flu-associated deaths, with also the same proportion having severe preconditions, resulting in 138 deaths of those otherwise healthy. Flu statistics are from the U.S. Centers for Disease Control's FluView.
Compared on a per capita basis, the U.S. exhibits a stunning 3.2 times death rate over Canada, either pre-compromised health or not. (Click chart to enlarge)
Since both countries promote flu vaccines, though declined by the large majority of citizens in both countries, and both exhibit similar flu rates, it is clear that Canada has essentially eliminated pediatric flu mortality, while something is terribly wrong in the U.S.
And, since the great majority of flu deaths occur after being hospitalized for days up to weeks, it's logical to review the treatment drugs and protocols and what is different between Canada and the U.S. An exhaustive review by this writer reveals two clear suspects, the antiviral drugs called ribavirin and oseltamivir.
RIBAVIRIN
The first suspect is a dangerous chemotherapy drug, called ribavirin, that has been increasingly used over the last decade in the U.S. for hospitalized cases with flu and associated respiratory infections, particularly the syncytial respiratory virus (RSV).
This chemotherapeutic drug has brand names of Virazole, Copegus, Rebetol, and was initially synthesized in the 1970's to investigate its use for cancer treatment when the War On Cancer investigated cancer-attacking therapies. Though never used for cancer, ribavirin was found to have extensive in-vitro (in the laboratory petri dish) action in stopping replication of various viruses. It is a nucleoside analogue and not only does it inhibit viruses, in human cells it takes the place of DNA chain links called guanine and adenosine. When a human cell tries to divide by replicating its DNA for a new cell, ribavirin substitutes itself and very effectively stops the DNA replication, thus aborting the new cell (and the parent cell dies also). This is how chemotherapy typically works when used for cancer treatments, though ribavirin's exceptional cell-killing action takes place throughout the entire human body more than most.
For many decades, a frequent co-infection of flu found in both infants and elderly called respiratory syncytial virus (RSV) has been found in flu patients, and starting about a decade ago ribavirin became increasingly recommended for RSV by various authorities including Aetna Insurance, The American Heritage® Stedman's Medical Dictionary, the Second Edition, and Dorland's Medical Dictionary for Health Care Consumers. To this writer, there is no justification for these recommendations, but an example of one writer following another and never checking basic toxicity studies.
Pertinently, ribavirin is also known as the drug of choice (given with interferon) to treat Hepatitis C, again because of its antiviral properties. But, this use is for short treatments as even ribavirin proponents acknowledge its many dangers, particularly dose-sensitive hemolytic anemia, hypoxia, and cardiac arrest via destruction of red blood cells. Of the estimated 8,000 annual U.S. Hepatitis C deaths, many may be directly or in part from the treatment itself as this writer can testify with family experience in the matter.
As for ribavirin and RSV frequently associated with flu, health care professionals increasingly go to medical websites, and WrongDiagnosis.com is one of the world's leading providers of online medical health information (they say so themselves). According to WrongDiagnosis they are an independent, objective source of factual, mainstream health information for both consumers and health professionals. Here is what WrongDiagnosis.com says about ribavirin for RSV:
"Among the goals of treatment are support of respiratory function, maintenance of fluid balance, and relief of symptoms. Mild cases resolve without treatment. Severe infections require hospitalization to provide supplemental oxygen, humidified air, and hydration by I.V. fluids. Respiratory support using mechanical ventilation may be needed. Ribavirin aerosol may be used in those who have severe RSV or are immunocompromised."
However, here is what is found on WebMD, sponsored by the entity RxList:
"Deaths during or shortly after treatment with aerosolized Virazole have been reported in 20 cases of patients treated with Virazole (12 of these patients were being treated for RSV infections). Several cases have been characterized as "possibly related" to Virazole by the treating physician; these were in infants who experienced worsening respiratory status related to bronchospasm while being treated with the drug."
So, American providers may employ ribavirin depending on their reference source and habit. But, do Canadian doctors ever use ribavirin for RSV, flu-associated or not? A representative answer comes from the Province of British Columbia with their health site called HealthLinkBC (their term "very rarely" basically means never):
"Ribavirin (Virazole) is an antiviral medicine that is very rarely used to treat people with RSV infections who have a high risk of developing complications. Studies so far have provided conflicting evidence regarding its effectiveness. The doctor will consider the particular circumstances of the person being treated before making a recommendation about ribavirin."
The 2003 experience of doctors in the Canada Province of Ontario is telling, and their experience with ribavirin is crucial. Canadian doctors in Toronto hospitals gave strong doses to virtually all patients during the 2003 SARS Panic that had seized the medical world. SARS was defined as being mild pneumonia symptoms and having contact to SE Asia, initially thought caused by a mutated corona virus (later disproven). After experiencing quickly rising hospital deaths, and belatedly realizing hemolytic anemia symptoms were caused by ribavirin, Canada authorities blew the whistle and stopped its use, and deaths quickly fell off.
Not by coincidence, not a single American died of SARS and there was only a single death in all of Europe, as all respective health authorities declined the use of ribavirin. All other SARS deaths (but one in South Africa) took place in SE Asia and China with extensive documentation of patients strongly dosed with ribavirin. Even more telling, one Chinese Health District did not use ribavirin and had no mortality, while in contrast neighboring Districts using ribavirin recorded significant mortality. The total SARS deaths were 43 in Canada, 1 in Europe, 1 in South Africa, and 738 in SE Asia and China.
Learning their lesson from SARS, Canada's doctors have apparently taken it to heart, and it seems extremely unlikely their RSV treatments include the chemotherapy ribavirin, unlike apparent widespread use in the U.S. Flu deaths in both Canada and the U.S. are almost all listed as flu-associated and one of these associations is RSV. With Canada averaging but one pediatric flu-associated death a year (of those previously healthy), they certainly are doing something right.
OSELTAMIVIR (TAMIFLU)
The second questionable drug affiliated with U.S. pediatric flu death is oseltamivir, also known as Tamiflu, another antiviral drug effective in a petri dish against virus replication. The petri dish is one thing, but its cellular toxicity in humans is another, and makes this writer question any legitimate use. There is a wealth of evidence citing its dangers.
For instance, in 2007 Japan authorities banned Tamiflu after determining it was THE causal factor in teenager suicides, and in August, 2009 the UK's Telegraph news reported there were 400 cases of significant Tamiflu side effects as many panicked by the Swine (H1N1) flu rushed to take the antiviral medicine.
Despite the U.S. CDC saying Tamiflu was marginally effective (if at all) when quickly used at onset of flu symptoms, medical records show it is inexplicably employed continuously until a patient is either discharged, or dies. This is specifically documented in the MMWR weekly report of September 4, 2009 with a chart of 36 pediatric deaths showing every death but one after a hospital stay (involving at least an overnight admission to the ICU) was in all likelihood continuously treated with oseltamivir or other antivirals at unspecified dosages. (See: HERE. ) However, adult fatality case reports cite double-strength oseltamivir dosing, an ominous clue that suggests what may also be happening in pediatric patients.
FLU VACCINATIONS
Since flu has been convincingly demonstrated by Canada to be of minimal risk to kids, it makes sense to seriously question the safety and risks of flu vaccines.
Flu vaccinations are endlessly promoted and the U.S. CDC has for years designated the first week of December as National Flu Vaccination Week, with countless media promotions and the CDC press releases in the news. However, news of Canada's next-to-zero flu toll is unknown to the American public. Also ignored by U.S. media (and apparently by CDC) is recent dramatic news from Australia.
Australia's ABC News reported April 23, 2010 that seasonal flu vaccines for young children had been deemed too dangerous with reactions greatly under-reported, and Australian doctors have now been warned not to give the seasonal flu vaccine to children under the age of five, after a child fell critically ill and dozens more suffered serious adverse reactions after receiving the vaccine in Western Australia, with The Australian Medical Association backing this move to suspend vaccinations in children under five around the entire country.
Canada's paediatric group averaging a single flu-associated death per year the last four years strongly questions the sanity of promoting a mercury-laden flu vaccine jab that also brings many other toxic ingredients such as aluminum-compound adjuvants and many other alien substances into cellular contact of fragile developing neurological systems, particularly infants and kids as young as six months.
It is vital to note Canada's minimal flu toll takes place while many are actually declining the vaccine jab. From the April 21, 2010 Times Colonist in British Colombia comes "Only 40 per cent of B.C.'s population chose to be vaccinated against H1N1, which meant roughly 2.5 million of the 4.3 million doses ordered by the province were not used, said Ida Chong, minister of healthy living and sport." Importantly, all of Canada (except New Brunswick)* called off the seasonal jab in lieu of the H1N1 jab, thus eliminating the role of multiple flu shots. *(See HERE for a May 17 post by this writer on New Brunswick advocating both seasonal and H1N1 flu shots, resulting in much higher sickness rates).
So, Canadians by a wide margin refuse flu vaccines yet have but one flu-associated paediatric mortality a year, as close to zero as it gets. From this writer's perspective, the documented risks of flu vaccine can be dire and deadly, while the jab's benefit is an illusion wrongly promoted by evidence also as strong as it gets. To wit: the U.S. vaccine adverse event reaction system called VAERS from September 2009 to the present recorded 16,982 flu-vaccine reactions among all ages. But this is just the tip of the iceberg, as experts have long stated at most 10% adverse reactions are actually recorded in the VAERS database.
Canada's doctors have figured out flu treatment and the hazards of the chemotherapy ribavirin by the School of Hard Knocks, while Australian doctors have blown the whistle about extreme flu vaccine dangers to their kids. Meanwhile the U.S. public is kept in the dark, exhorted to take 6-month old infants to be vaccinated, and further having them treated by medical protocols using pervasively deadly ribavirin created for cancer chemotherapy, and/or with copious doses of toxic Tamiflu.
How can U.S. Health Generals and mainstream media not notice Canada's weekly reports having identical record-keeping as the CDC? Or, pay attention to Australia's warning with their flu season preceding the U.S.? Or review and report objectively the unambiguous dangers of antiviral drugs?
Instead, health officials are typified by their CDC spokeswoman nationally broadcast last October on National Public Radio stating "mercury in flu vaccines poses absolutely no risk to infants and children" -- a statement that left me speechless then, as it does now.
David (DB) Burd's professional experience spans four decades of technology innovation, design, and trouble-shooting with various engineering firms, and has concentrated the last decade on medical technology and related topics after experience as a U.S. patent examiner in medical technology. DB's corporate and consulting activities followed an initial eight years of positions in the national defense arena. DB was in the first graduating class of "rocket scientists," with a BSME in Mechanical Engineering and Astronautical Sciences from Northwestern University. DB also writes on medical topics, and provides analytical expertise to organizations involved in major public health issues.